
Feminizing HRT
What interventions are needed for feminizing effect?

Day 22/30 of posting daily
TLDR: taking a weekly injection of estradiol enanthate is the best option, taking bi-weekly valerate is a close second, but there are other options too.
This is a brief dump to try explain the main HRT methods. There are are better guides for this, such as this one, but for completion, I include some discussion here as well. Thing here are a mix of paper-backed evidence, as well as common-knowledge best things, and also some more anecdotal things too.
This mostly considers that you have standard reactions to HRT, but it is also quite common for this not to be the case for people with gender disphoria. I will discuss potential things to consider if you have weird genetics in a different post.
Best resources:
Here are a few of the best links for learning more (some others below too1)
https://trans.diy/feminizing
https://old.reddit.com/r/TransDIY/wiki/index#wiki_transfeminine
Goals of Feminizing HRT
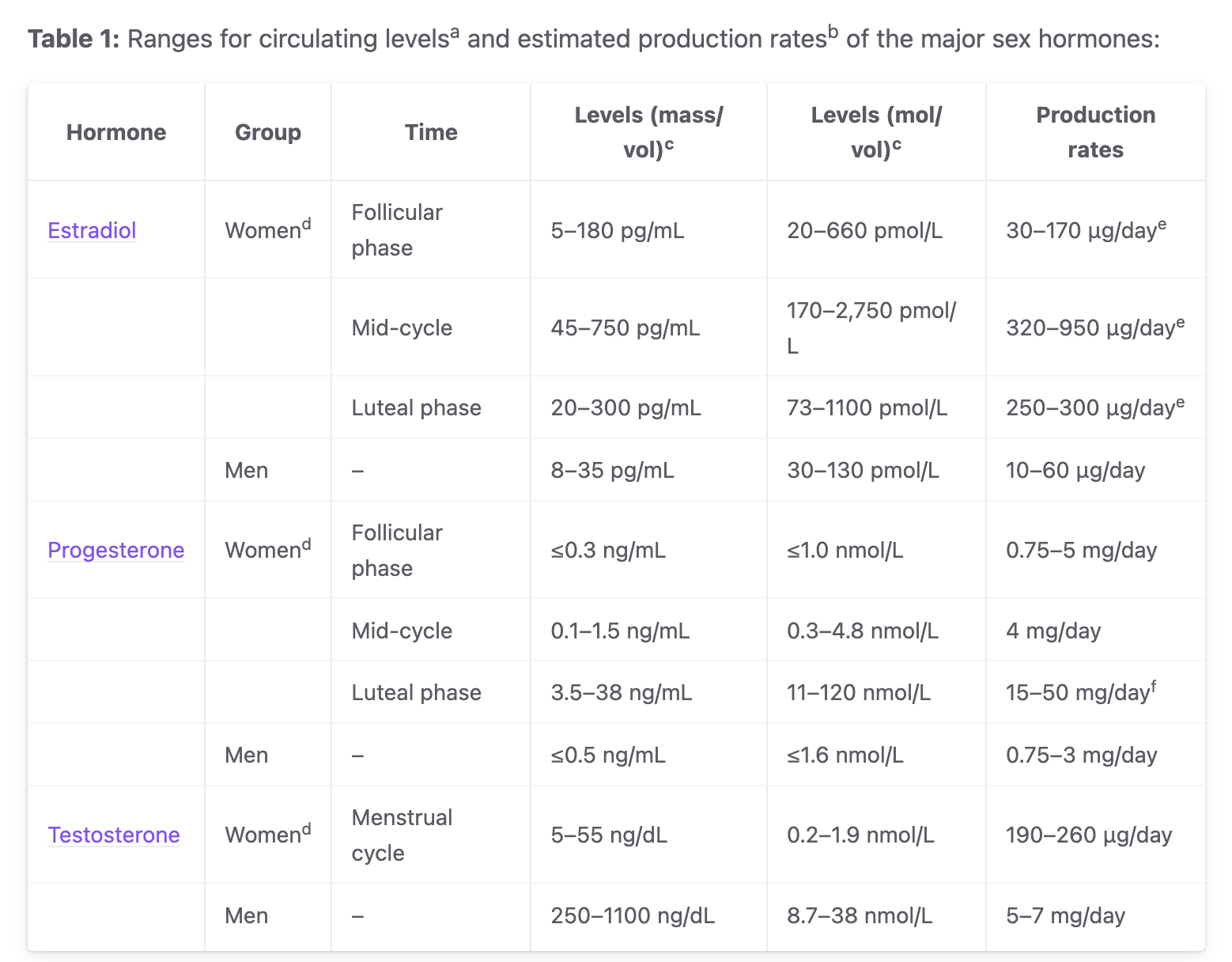
The main goal is to alter blood hormone profiles to match female hormone patterns. This means raising estrogen, and to decrease testosterone function. To some extent, the hardest part is making sure testosterone is low enough, as it’s effects are more potent than those of estrogen. Modifying progesterone levels can also help in later stages of feminization, though it’s effects are more debated.
The key axes you can use to modify things:
Estrogens
Anti-Antrogen
Progesterone
Non-hormonal
If you manage to get testosterone down under control, you want to make sure that your estrogen levels are high enough. Otherwise, you may get menopausal symptoms.
Anti-Androgen
This is the most important part to get right. There are a few ways to lower testosterone which I will mention, you may want to do your own research on side-effects and risks.
High estrogen levels
The simplest “anti-androgen”, is by having sufficiently high estrogen levels, that your body stops producing testosterone or estrogen on it’s own. This is only achievable with some methods of estrogen admission, which I will discuss later. This is my personally preferred method.
GnRH-Agonists
GnRH Agonists (and Antagonists2) are the most modern class of drugs for controling hormone levels.
This is a whole class of drugs, and ranges from pills, injectables and implants. The most easily obtainable being Relugolix pills, but depending on where you live you, medical systems can prescribe injectibles (such as triptorelin 3.75 mg/month or goserelin 3.6 mg/month) or by multi-month implants too.
These are the most effective and have the fewest side-effects compared to other methods, but are also more expensive, so are often not used as a first-line.
Bicalutamide
Bicalutamide is a non-traditional anti-androgen. It acts by blocking testosterone receptors rather than by lowering testosterone production, and thus often can lead to a rise in testosterone but a lowering in effects.
It is generally quite safe, there is some very rare liver risks (~1 in 1000) so you should take a couple of blood tests the first year or two that you use it to check for this, otherwise you should be fine. The elimination half-life is also relatively long (~1 week) so dose timing is not as important, typically it’s taken daily.
It is the best method if you can’t do the other methods, and has potential use as a non-binary HRT as I will discuss in a different post.
Cyproterone Acetate
This is another anti-androgen, that primarily acts similar to a progestin that blocks testosterone production and leads to lower testosterone levels. It has more potential side effects than previous options. It does slightly prevent testosterone receptors but is wak, . Normal dosing for feminizing is around 12.5mg/day or per 2 days.
It has some potential mental side effects, prolactinomas, liver toxicity, and mental effects. For this reason was not allowed by the FDA in the US through official channels, but it is one of the most common anti-androgens in the rest of the world.
Spironolactone
This is the weakest / worst anti-androgen that is prescribed, in doses of 100-200mg/day. It has relatively limited and inconsistent effects on testosterone levels in clinical studies. It is also a diuretic and makes people need to pee more.
It is seen as benefical to supplement B12 if you take spiro.
Other Anti-androgens
There are also a few others that are also work as anti-androgens, but don’t lower testosterone levels much / at all. You can see more in Retaining Head Hair post (which also includes discussion on Minoxidil)
Finasteride
Finasteride is typically only given as a DHT blocker In larger doses, of 5mg, it has some slight testosterone blocking effects too. Not typically enough to lower testosterone to female ranges.
Dutasteride
Dutatsteride is another DHT blocker. It also does not typically affect testosterone enough to lower it to female ranges.
Estrogen Admission Methods
There are a few types of estrogen, for most people we are interested in the most potent form, 17beta-estradiol, but there are other forms too (estrone, estrione, 17-alpha-estradiol). I will mostly only discuss the main kind of estradiol today.
It’s also worth knowing that estradiol can come in esters. This means that there is a little tail attached to it, which helps it be dissolved more easily in oil. This ester tail gets removed after entering the bloodstream, and thus the esters end up being bio-identical.
There were, in the past, synthetic estrogens which had bad side-effects such as blood clots, such as Ethinylestradiol, which can have longer elimination half-lives, but which also lead to increased risk of blood clots and some rare adverse effects. These are typically not recommended, though some continue to prescribe it.
Medical systems are difficult to work with in this space, and can have arcane requirements, so it can be worth working with medical systems or pharmaceutical vendors from places other than your home country. You can often find communities in your local area who can give better guidance on best medical options.
Different methods need different
Injectable Estradiol
The highest-consistency form of estrogen is to directly inject an ester of estrogen either into fat under your skin (subcutaneous or subQ) or into your muscle (intra-muscular or IM). This then stays around for a while, and the ester of estrogen leaks out into your bloodstream over the course of days.
This is most recommended, as it leads to most predictable results, and most reliably can be used for suppressing levels without an anti-androgen.
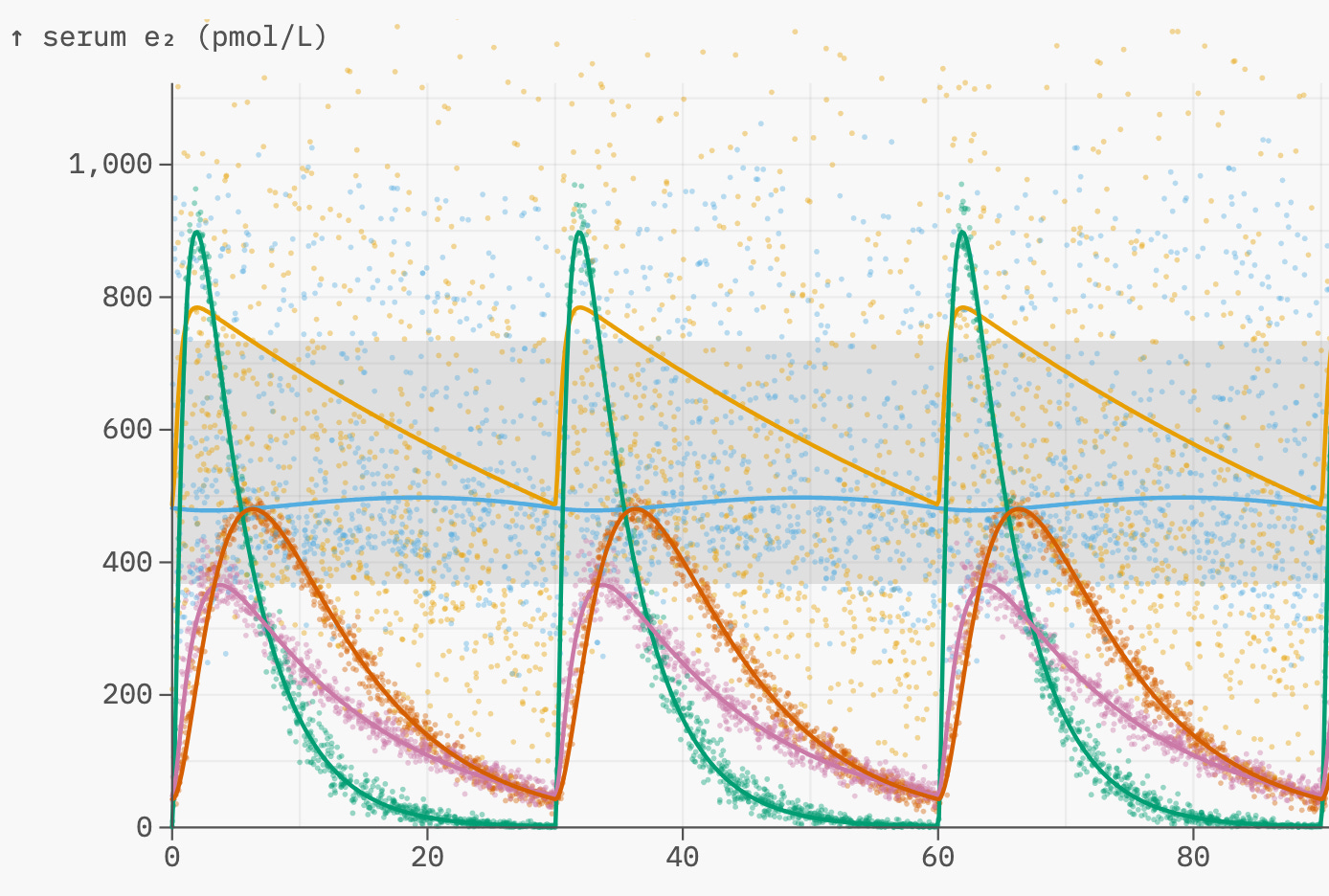
Based on estrannai.se, the half-life of esters are approximately:
estradiol valerate: ~4 days
estradiol cypionate: ~8 days
estradiol enanthate: ~7 days
estradiol undecylate: 20 to 30 days ish?
The best, most stable and reliable ester is Estradiol Enanthate. This can easily be injected once a week with relatively low spikes, and gives the most consistent levels from injection.
Estradiol cypionate is a close second, it’s slightly more “spikey” but has a similar half-life to enanthate.
Estradiol Valerate is one of the most common, as it is widely prescribed by medical institutions. It is significantly more “spikey” and has a shorter half-life, so is better to take on a 5-day or twice-weekly schedule instead of weekly.
Estradiol Undecylate has the longest half-life, around 20-30 days. This means it can be particularly useful as an option to take in advance of longer trips. However, it’s half-life is much harder to predict because there is less data, and there seems to be much more variance with what levels people achieve, and how it depends on carrier oil, etc.
There is non-zero concern that having slightly fluctuating levels of estradiol can be beneficial, but there is not much research into this.
Overall, Enanthate is probably the best option, or Estradiol valerate is good if it’s more accessible.
You can see guides online for injection technique.
Long-term Estrogen
It is possible to get Polyestradiol Phosphate intramuscularly, and Estradiol pellet implants implants, which can last for 3-6 months or so. These are quite uncommon, but can sometimes get directly from medical professionals in some countries.
Again, I have seen some little evidence that slightly fluctuating levels of estradiol can be beneficial, but there is not much research into this, so most likely you should not be too concerned.
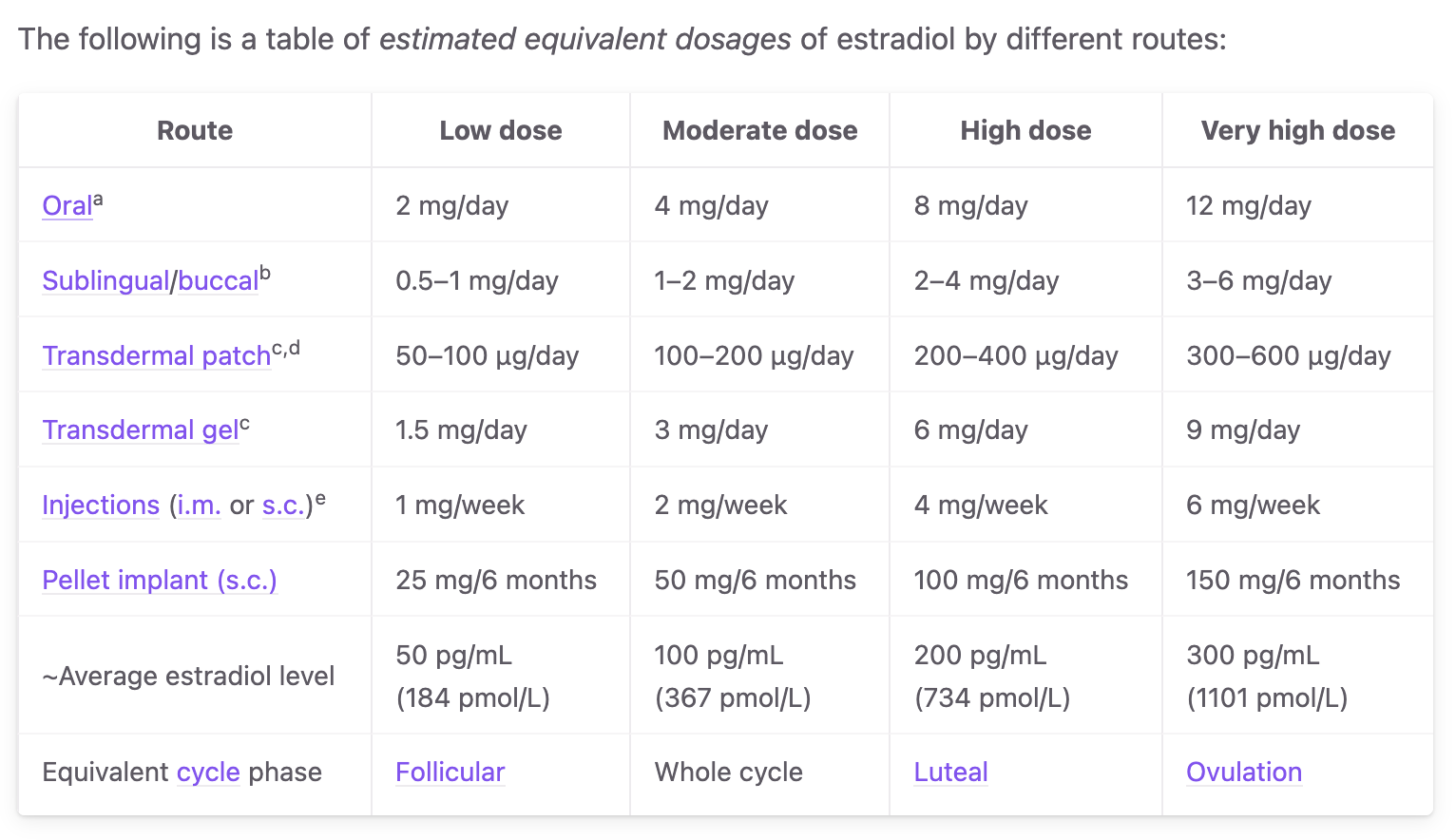
Estradiol Transdermal (Gel / Patches)
Applying Estrogen transdermally (through the skin) is the next best way to achieve high estrogen levels. It is, however, much less consistent with dosing than with injections. It is sometimes possible to achieve mono-therapy this way, though an anti-androgen is recommended.
You can either get patches, or put on gels. Either option is fine.
If using a gel, site of application alters absorption significantly. Highest absorption but also highest variance is application to scrotum. Application to the chest is not advised due to potential breast-cancer risks.
Estradiol (Oral / Sublingual)
It is also common and possible to take estradiol orally or sublingually.
Sublingual (under the tongue) is generally much better as absorption can be significantly higher, 2-4x more.
With orally taken estradiol, it is typically not possible to reach mono-therapy levels, as it gets processed by the liver before entering the bloodstream. Thus taking an anti-androgen is advised.
Estradiol Stickies
If you have a limited supply of estrogen, then it is possible to create stickies that only need 0.4mg of estradiol per day. See this interesting description to learn more
Progesterone
The last main hormone that varies in women is Progesterone. You can read this paper on it.
There is evidence to suggest this is helpful for advancing breast growth from earlier stages to later stages (causing the breast bud ducts to mature). This it is typically better to start this much later in transition.
The two main methods of administration are:
orally (taking around 200mg), though most of this gets converted to allopregnanolone, and only a small fraction remains as progesterone. Allopregnanolone typically makes people sleepy, so people sometimes take it before bed.
boofing, administering rectally daily makes it easier to absorb higher levels without being converted to allopregnanolone.
It is possible to get injections of progesterone, but the half-life is much shorter, and it’s not as important as estradiol. This, most people don’t find that it’s worth ~daily injections and it is not particularly commonly prescribed.
There are some gel recipes for progesterone too, but these have not been tested that much either.
The main issue, is that it is not possible to easily add an ester to progesterone, and only synthetic progestins are common. However, these are associated with bad side effects and are not particularly safe to take long-term.
Other compounds
Pioglitazone
Another drug, as mentioned in “gaining fat in the right places” is pioglitazone. This has been shown to somewhat improve feminine fat distribution and promote the creation of fat cells. It is somewhat recommended to only take this after you have already been on HRT for a while.
Domperidone
This is another drug that can be used to induce lactation, and can lead to larger breasts while taking the drug. It is probably better to not take this too early on in transition. It may have some risks too, so you should look into those.
This is typically only used to treat nausea, and the lactation is more of a side-effect, so it’s not commonly prescribed.
Final Thoughts and Other Considerations
There is a lot of research into these various compounds for femenizing HRT.
One default that doctors like to err towards, is to have the minimal possible amount of estrogen that leads to feminizing effect, and often start with prescribing placebo-level doses. However, the risk of high-estrogen levels is not particularly with non-orally administered bio-identical estrogen (other than some possible increase in breast-cancer risks over very long periods of time), so you may want to consider starting at a higher dose and working down, as time on a sufficient level of HRT is what leads to results.
You also might want to consider that many people with gender dysphoria often have some abnormalities in their processing of hormones, in their testosterone and estrogen receptors. You may want to try different things if this is the case, rather than blindly increasing estrogen levels. I will write about this more a different day.
It may be worth looking at my weight-cycling series for some more info on that too.
I will probably spend another day discussing non-binary HRT and masculinizing HRT as the requirements for these are different.
https://apps.carleton.edu/campus/gsc/assets/hormones_MTF.pdf
https://www.rainbowhealthontario.ca/TransHealthGuide/gp-femht.html
https://en.wikipedia.org/wiki/Feminizing_hormone_therapy
https://www.hormonebalance.org/images/documents/Kuhl%2005%20%20Pharm%20Estro%20Progest%20Climacteric_1313155660.pdf
Both GnRH Agonists and GnRH Antagonists tend to lead to the same continuous long-term suppression, though initial effects from the first few hours can differ. I don’t fully understand why.