
Retaining Head Hair
Preventing Balding


Most people do not want balding on their head.
If you are a man, you have high testosterone levels may also lead to downstream balding too.
If you are a woman, and transitioned only when you were older, you may have experienced some balding.
I will try to explain what causes balding, and some interventions you can do to try to prevent it.
What causes Male Pattern Baldness (MPB)?
There are a few kinds of balding, but the most common kind is called androgenetic alopecia (AGA), which is seen as Male Pattern Baldness (MPB). It is highly heritable.
Testosterone in the blood is converted by the 5-alpha-reductase (5-AR) enzymes into DHT. (there are 3 types of 5-alpha-reductase). This then causes balding in some, depending on genetics.
The typical pathways differ:
The most common genetic factor, is that your follicles become more sensitive to dihydrotestosterone (DHT).
For some, the DHT just causes more growth inhibitors locally.
For some, some DHT production is locally higher at the scalps.
DHT Is also responsible for stimulating facial and body hair growth, but in adulthood is not that responsible for that many other things.
This, one key pathway to preventing Male Pattern Baldness is to prevent DHT.
Other factors?
Some other factors that can also increase the chance or severity of balding:
Smoking might increase risk. One study showed it increased the chance of MPB by about 2x compared to non-smokers, but I have not read broadly here.
Sleep, stress, insulin resistance, and dermatitis can maybe affect things, though the effect seems likely not that big from most of these. I haven’t read much here.
Diet can matter, if you are deficient in some nutrients that can sometimes cause balding too.
But these are not usually the main factors
Norwood Scale
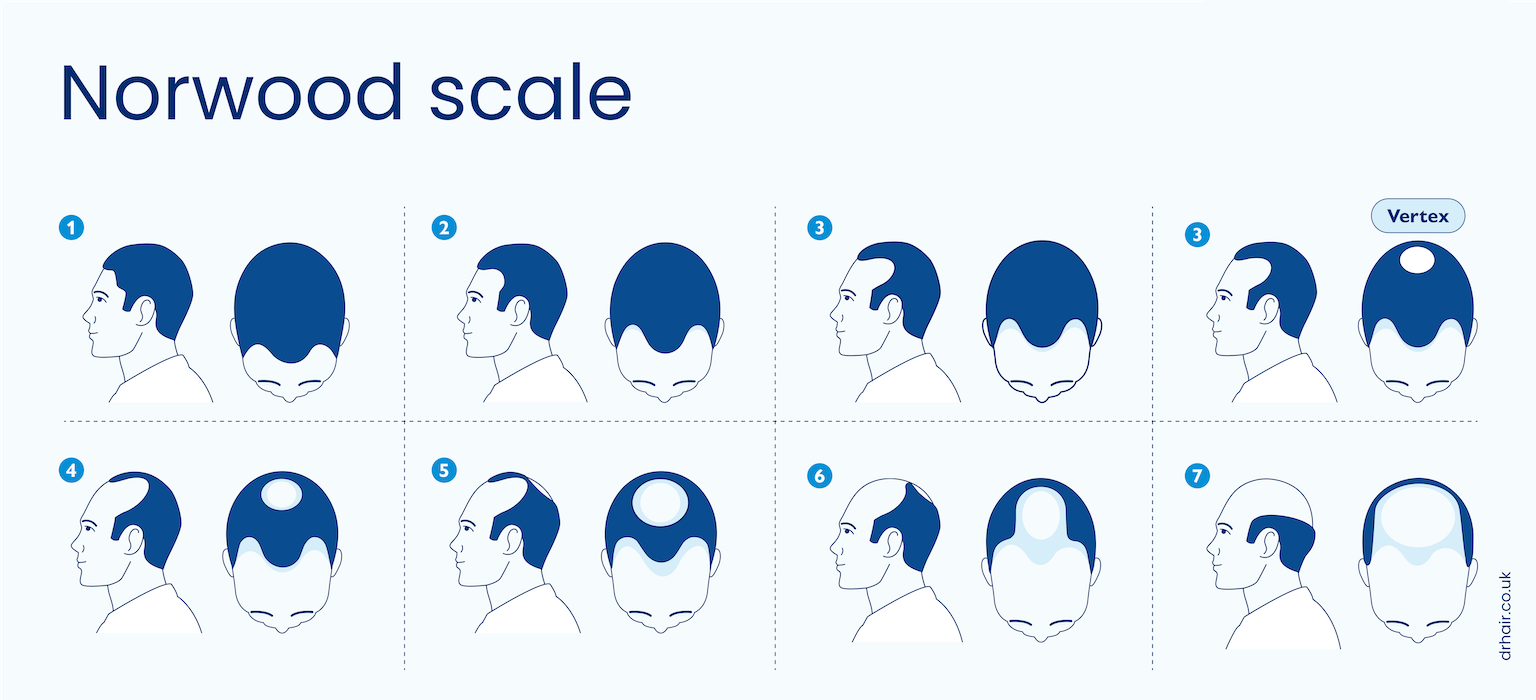
It’s worth briefly touching upon the Hamilton-Norwood Scale. It shows the progression typical for Male Pattern Baldness (MPB). You can see the diagram above. It is common to describe your hair as having a certain level of MPB, such as “Norwood IV”.
The Standard Recommendations
The most typical recommendations to try to prevent balding, is to use a DHT blocker such as finasteride/dutasteride, and/or to use minoxidil. I will discuss these somewhat below.
Finasteride
The most common prescription, is to take 1mg of finasteride orally daily. It has a half-life of about 6 hours.
This primarily acts on inhibiting 5-alpha-reductase type 2.
This then means that scalp DHT levels drop by about about 64% on average, enough such that for most men, hair loss is halted.
One hope for some amount of regrowth, but it’s mostly the case that only hair lost in the past few years will grow back.
Risks?
There are non-zero risks for men, but they are quite small. Erectile dysfunction increases from ~0.7% in the placebo to 1.3% in the active group, and gynecomastia risk increases from ~0.1% to 0.4%. I overall count this as not significant and pretty minor.
Topical Finasteride
Alternatively, one can apply finasteride topically. A 0.25% solution of finasteride spray applied once daily is non-inferior to 1mg of oral finasteride, but has a less significant drop in serum DHT (~34% vs ~56%).
Dutasteride
An alternative to finasteride to have stronger effects, is to take dutasteride. This blocks all three 5-alpha-reductase receptors (though type 3 to a lesser extent), and also has a longer half-life (~4 weeks instead of 6 hours).
While people can take 5mg finasteride, the difference in DHT is not big compared to 1m doses, but it does have more side effects.
Instead, 0.5mg dutasteride reduces DHT by about ~92%.
There is, however, more chance of adverse sexual effects with dutasteride too.
Minoxidil
The last common treatment discussed is minoxidil, typically taken as a 5% topical solution applied to the areas where you want hair to grow.
Effectiveness of minoxidil is somewhat variable and depends on genetics. You need to have SULT1A1 enzyme activity for it to work.
The way it works is more complicated than I have time to describe rn, but I will maybe come back to it at some point.
Oral minoxidil
It is also possible to take minoxidil, and 1mg of oral has been shown to be similar in effectiveness to 5% topical on some axes, but it’s much less studied, so I’m not sure
Risks
Minoxidil can be fatal for pets
It can also cause hair growth in undesirable locations if you let it drip
Other Considerations
If you have low testosterone, this should already cause you not to produce DHT. It is possible to to have other kinds of balding, but I will discuss those some other time maybe.
Other Topical Solutions
These are some alternatives have more limited evidence:
Ketoconazole 2% shampoo might work
Topical 17-alpha-estradiol might work, used moreso for female pattern baldness though.
Here are some other compounds that are still undergoing clinical trials, but these topical solutions have had some promising results:
Clascoterone 5% topical (Breezula)
GT20029 (Kintor)
Pyrilutamide / KX-826 (Kintor)
Actual recommendations?
It may be worth doing a genetic test to see whether you are at risk of male pattern baldness. If you are not, then there is no need to do any of these steps. This can be expensive, but is getting cheaper every year. Alternatively, you can just look at your family history to get an idea, or notice if you have any changes to your hairline.
If you do want to take these steps, it may be worth doing a Prostate-Specific Antigen (PSA) Test, in order to have some baseline, especially if you have a prostate and are at high risk of prostate cancer, and are not sure if you want to do full feminization. But if you do decide to transition, then you don’t really need to worry about it.
Otherwise, the standard recommendation, is to go:
start with 1mg finasteride taken orally daily.
If you prefer a topical solution or want to double up, you can go:
5% topical minoxidil daily
You will need to take at least 6 months to see if it’s working. If not, you may want to upgrade to to dutasteride.
There are other things, but I will need to add them at some later point.
I do wish I had taken finasteride earlier - for some reason I started with and stayed on minoxidil, which as I understand it is usually not sufficient to overcome the balding effects of DHT long term
probably worth mentioning that post-finasteride syndrome is a real thing and can be catastrophically bad even if it is rare.
i also think this post underrates topical fin/duta relative to oral. topical is safer since you get more into the follicles and less into systemic circulation.
i don't think there is a good consensus on whether fin or duta is better or in which cases. i don't think duta is necessarily "stronger" because you can take it at a lower dose to compensate for the longer half life and blocking both isozymes.
i think scalp massage helps both for absorption of topicals and also just increasing scalp blood flow (extends anaphase)