
Voice Surgery Techniques
Comparison of the main techniques and what aspects of voice they affect

Day 7/30 of Inkhaven. Writing every day to get information out of my head.
In yesterday’s post, I wrote about the main aspects of voice. Of course voice has many dimensions to it, but the three main physical aspects are: resonance, weight, pitch.
Testosterone during puberty directly causes the expansion of the vocal cords and larynx, and results in a deeper and heavier voice. Taking testosterone as a trans man also causes this to occur, but not everyone reaches the same end point (and much later after natural puberty can affect this), but taking estrogen as a trans woman does not cause the vocal cords and larynx to change back.1
Today I will discuss the main voice surgery types. The standard recommendation is to not get surgery, but if you do get surgery, the standard route is to get a vocal cord shortening procedure.
Surgery Targets
Surgery can affect a few different things.
The first is that it can affect the vocal cords, either by affecting the length of the cords, the tension, or the mass/stiffness of them. This has effects on weight and on pitch.
The second is that it can affect your broader larynx/voice box, and thus alter the size of your pharynx. This is intended to have some effects on resonance.
The last is that it can aesthetically affect the appearance of your Adam’s apple. It is not intended for this to affect voice quality.
You may like to refer to some of the parts of the mouth (not strictly necessary to know):
Vocal cords = the vocal cords which vibrate when you speak
larynx = the whole voice box including what is inside
Glottis = the middle laryngeal region that includes the vocal folds and the opening between them
pharynx = the throat behind your mouth/nose above your voice box
thyroid cartilage = the cartilage on the outside of your voice box
Types of Surgery
And there are different surgeries that affect the different aspects, categorized in 5 main ways:
Tracheal shave is the first kind, and is purely cosmetic. A properly done “chondrolaryngoplasty” is meant to be voice-neutral. But overaggressive reduction can destabilize how some things attach, and cause voice problems like lowered pitch or dysphonia
Tension-based procedures are the second kind (eg: ACA, CTA). These just try to “stretch” the vocal cords more tightly, and raise pitch that way. It does not affect vocal weight much, produces results that are strained and falcetto in quality, and also relaxes over time. This is an old type of surgery that has fallen out of favour.
Laser-based procedures are the third kind of surgery (eg: LAVA, LRG, VFMR). This tries to alter the the mass/stiffness of the tissue. However, it mostly alters the mass/stiffness of the vocal cords to be lighter, and sometimes tension2, but not length. There is a reduction in vocal weight and increase in pitch, but the effect is relatively small. It also typically causes a moderate reduction in quality and range. It is, however, relatively less invasive and does not require an external excision into the neck.
Shortening procedures are the fourth kind of surgery, (eg: Wendler Glottoplasty, VFSRAC). This primarily changes the length of your vocal cords, and by proxy also changes the mass and the tension in your vocal cords. It does not affect resonance, so still requires some voice training. It is is also less-invasive and does not require an external excision into the neck. Wendler gluttoplasty is the standard good kind of voice surgery people get these days.
The differences between Wendler Gluttoplasty and VFSRAC are notable, but relatively minor in practice. The former only cuts the vocal cords and re-attaches them together to be slightly shorter. The latter makes an additional to better control how mass+length+tension change. (It also makes it so that the tissue below the vocal cords also makes a slightly more “conic” shape rather than being suddenly smaller). There are some theoretical reasons this could be somewhat better, but I don’t fully understand them, and my understanding is that it’s not a huge difference.
Thyrohyoid Elevation (THE) is the fifth kind of surgery. This involves altering the cartilage of your voice box to be higher up and trimmed to be slightly smaller. This is the only one that affects the pharynx, and so affects resonance. This procedure, alone, does not alter pitch or weight, but is usually paired with shortening procedures. This surgery is particularly invasive and risky.
One notable surgery, is that one can get a FemLar, which is a combination of thyrohyoid approximation + vocal cord shortening + tracheal shave. This is the only method that results in a voice that requires the least amount of voice training in theory (though still requires training), and is also the single riskiest procedure.
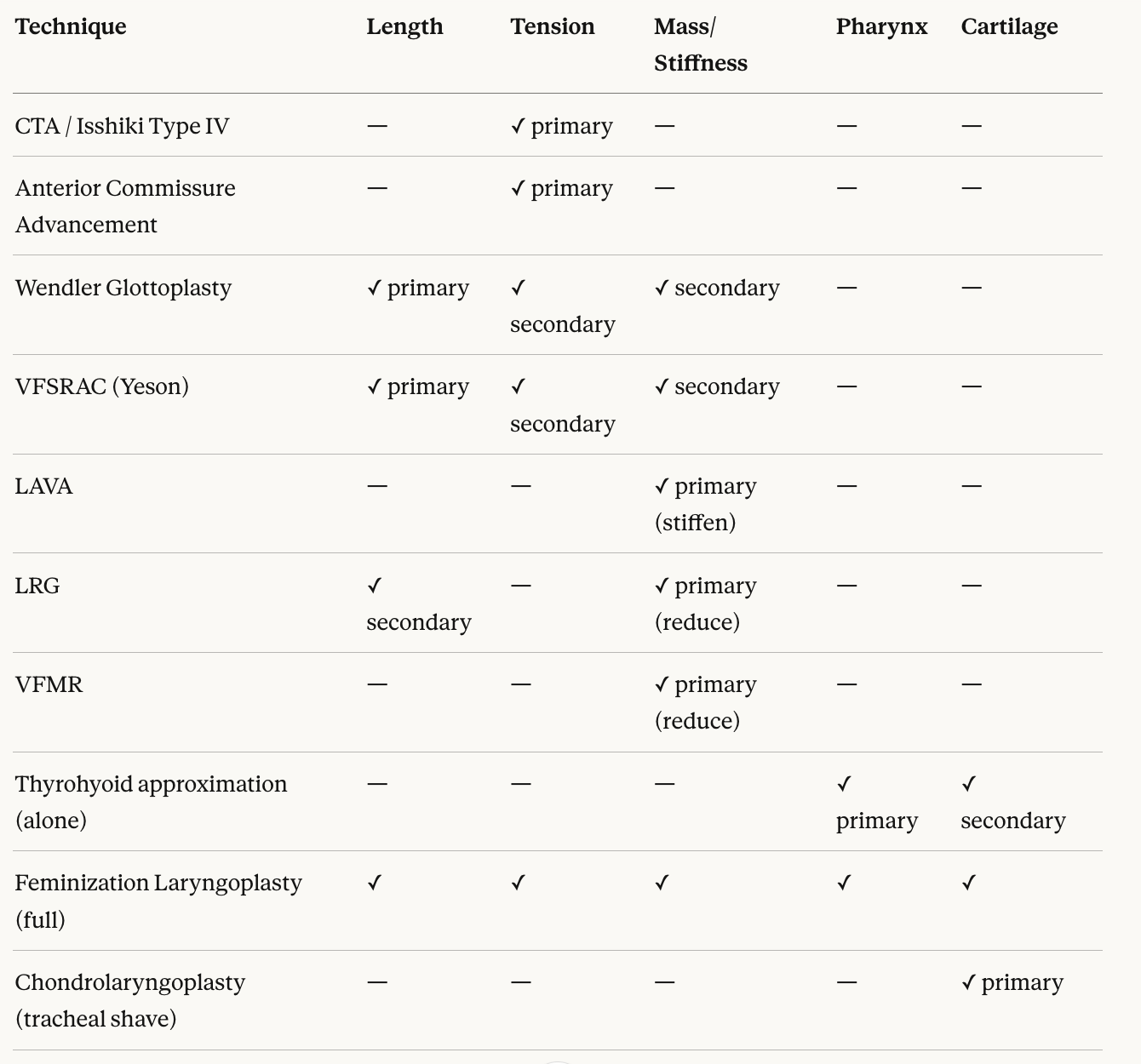
One can summarize the results as such:
Surgery Recommendations?
This is more opinionated than the sections before
Ideally, for most people, it is possible to achieve good results through voice-training alone with enough effort. It can be very difficult, but surgery has it’s own risks too. Most voice surgeries trade away some vocal flexibility (especially low range) and some can reduce loudness or alter quality, though the degree varies by procedure.
If you do choose to get surgery, my current top recommendation is to get shortening-surgery. This has the best tradeoff between how good the results are, amount of voice training needed, and how safe the procedure is. I personally went with Dr. Kim at Yeson in Korea, as he has done countless surgeries over the course of years, has published significant amounts of research, and trained many of the other best voice surgeons. But there is not much difference between Wendler Gluttoplasty techniques if they are skilled and reputable, and you may have tradeoffs in cost/insurance coverage/distance.
Getting a tracheal shave is slightly not recommended. But aesthetically, if you have a large Adam’s Apple or feel dysphoric about it, the risks are not that large and you should probably get it done. If you value voice quality above all, it may have some slight effect. It is typically recommended to get it after VFS, but you can get it before too. Either way, let your FFS know the guidance from your VFS surgeon.
If you care only about the best-case-scenario for voice and don’t mind a pretty large risk of things turning out bad, it is possible to get really excellent results through FemLar. I don’t personally think the tradeoffs are worth it, but this is the most comprehensive, but risks damaging your voice more.
In a future post, I will talk about the experience getting Yeson VFSRAC.
Technically, there is some effect on vocal aspects from difference in hormones, such as differing hydration levels altering the mucus. But the effects are quite minor and not really that noticeable.
LAVA is usually described more as stiffening / altering the vibrating membrane than simply “making weight lighter,” while LRG/VFMR remove tissue more directly.